
Demonization of women who use substances while pregnant has resulted in law enforcement policies that may have caused further harm. In the 1980s, during the “crack-cocaine” crisis, the U.S. government shifted drug control efforts from health to criminal justice in what was called the “War on Drugs.” Some of the resulting policies led to women being incarcerated, forcibly detained in treatment facilities, or losing their children. The fear of facing these punitive measures can discourage women from seeking care (Bishop et al., 2017). When laws fail to consider the underlying reasons for substance use disorders, unintended consequences can negatively affect overall health including reproductive autonomy.
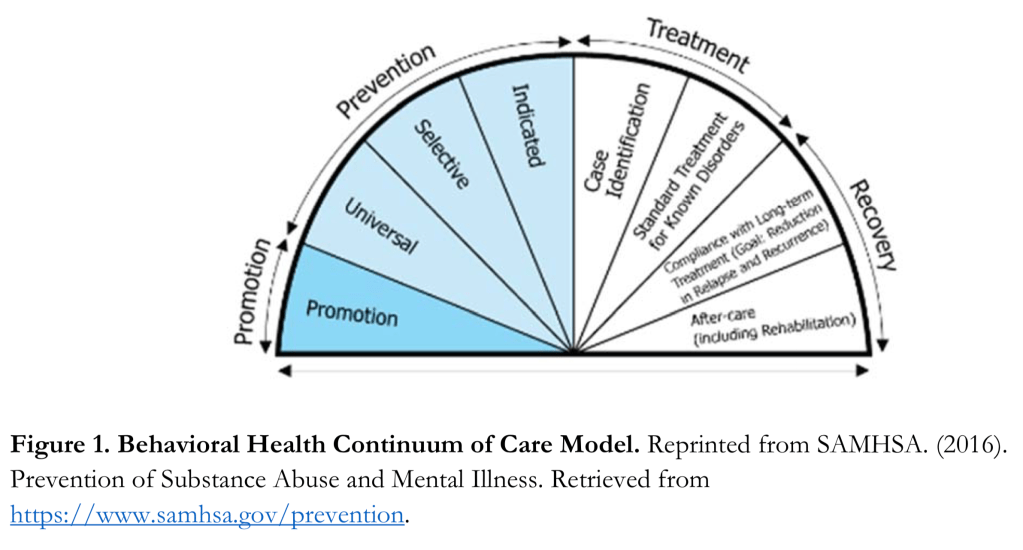
A public health approach works to encourage and assist women to gain access to needed treatment and care. The public health focus favors harm reduction over punishment. Public health also focuses on prevention. Such strategies include access to substance use treatment for women of reproductive age and women-focused services in recovery programs. One government agency that works toward this goal is the Substance Abuse and Mental Health Services Administration (SAMHSA). According to SAMHSA, approximately 8% of Americans have a substance use disorder (SUD). SAMHSA’s Behavioral Health Continuum of Care Model promotes a more holistic view for addressing substance use from a mental illness perspective.
Fortunately, there are current efforts to address the opioid-related crisis that have learned from past policies and are focusing more on treatment instead of punishment. However, while the large majority of SUD programs accept women as clients, only a minority offer programs designed for women despite research showing that women are more likely to enroll and remain in programs that are women-centered (Bishop et al., 2017).
While women with SUDs struggle to find programs tailored for them, another force is acting against their reproductive equity. The battle for reproductive autonomy and access to quality family planning is affecting all women in our nation. Title X is a United States Department of Health and Human Services (USDHHS) funding program that provides family planning grants to health departments, public and non-profit agencies and community centers (USDHHS, 2019) that has suffered regulation changes swayed by the Trump administration (Kingdom, 2011; Sonfield, 2018). Title X is an example of regulation change that has come from the conservative attempts to restrict reproductive autonomy, particularly abortion. In doing so, access to pregnancy prevention and preconception health care will also be restricted.
Power to Decide is a private, non-profit agency that promotes a person’s right to determine if when and under what circumstances they would like to become pregnant. Power to Decide is an active voice in policy-maker ears to support women’s reproductive autonomy. Power to Decide projects more “family planning” deserts will arise as a consequence of the Title X changes.

In order to reduce unintended pregnancies or to improve the health of desired pregnancies among women in recovery from substance use disorders, we need policies that make it easier for women with substance use disorders to access family planning, not more difficult. Policies and programs are needed to promote more women-focused SUD programs that provide integrated, holistic services.
Exchange of accurate scientific and clinical information between researchers and policy-makers has the potential to ensure that policies are grounded in the best available evidence. Making the connection between policy and science is critical if we are to promote women’s health through improved access to high-quality healthcare.
Jacobs Institute of Women’s Health Bridging the Divide (Bishop et al., 2017)
References
Kingdon, J.W. (2011). Agendas, alternatives, and public policies.(2nd ed.). Glenview, IL: Pearson Education Inc.
Sonfield, A. (2018). Trump administration revives Title X ‘domestic gag rule’. Contraceptive Technology Update, 39(8).
US Department of Health and Human Services (2019). Compliance with statutory program integrity requirements: Title X program guidance. Retrieved from https://www.hhs.gov/opa/title-x-family-planning/about-title-x-grants/statutes-and-regulations/compliance-with-statutory-program-integrity-requirements/index.html

Thanks for your interesting blog. I am very convinced that changes in health service policies for pregnant women struggling with substance use disorder (SUD) will impact the outcome of women’s health, recovery, and rehabilitation from substance use. Access to health services specifically family planning services for women struggling with SUD are of utmost importance because pregnancy along with SUD can jeopardize the recovery from drugs. Substance use during pregnancy can lead to long-lasting consequences including fetal alcohol syndrome, stillbirth, and miscarriage (Substance Abuse and Mental Health Services Administration [SAMSHA], n. d.). I appreciate your endeavor and advocacy for such an important policy for women’s health and wellness.
Reference
SAMSHA-HRSA Center for Integrated Health Solutions. Substance Use Disorder and Pregnancy. Retrieved from https://www.integration.samhsa.gov/about-us/integration-edge/substance-use-disorder-and-pregnancy
LikeLike
Karen,
Thank you for your informative blog. Women with substance use disorders (SUD) experience a high rate of unintended pregnancies and should be offered contraceptive counseling and access to contraception (American College of Obstetricians & Gynecologists [ACOG], 2017; Substance Abuse & Mental Health Services Administration [SAMSHA], 2018). Women with SUD who present for prenatal care should receive counseling regarding postpartum contraception should be a part of routine prenatal counseling. Improving access to standardized evidence-based treatments for SUD will help to improve long term outcomes for these women (SCOG, 2017; SAMSHA, 2018). Providers should educate themselves about available treatments within the community. Speaking up to healthcare policymakers to improve overall healthcare available to women will help to improve access to care and also decrease health disparities that may be present for women with SUD.
Brittany
References
American College of Obstetricians & Gynecologists. (2017). ACOG committee opinion No. 711: Opioid use and opioid use disorder in pregnancy. Obstetrics & Gynecology, 130, e81-94. doi: 10.1097/AOG.0000000000002235.
Substance Abuse and Mental Health Services Administration. (2018). HHS Publication No. (SMA) 18-5054: Clinical guidelines for treating pregnant and parenting women with opioid use disorder and their infants. Rockville: Substance Abuse and Mental Health Services Administration.
LikeLike